
Sticker Shock
What nobody tells you about health insurance when you’re building a business.

There’s a moment every growing business owner hits.
You’ve got real revenue. Maybe a team. Things are starting to feel like a business — not just a hustle with a bank account. And then someone says the words: health insurance.
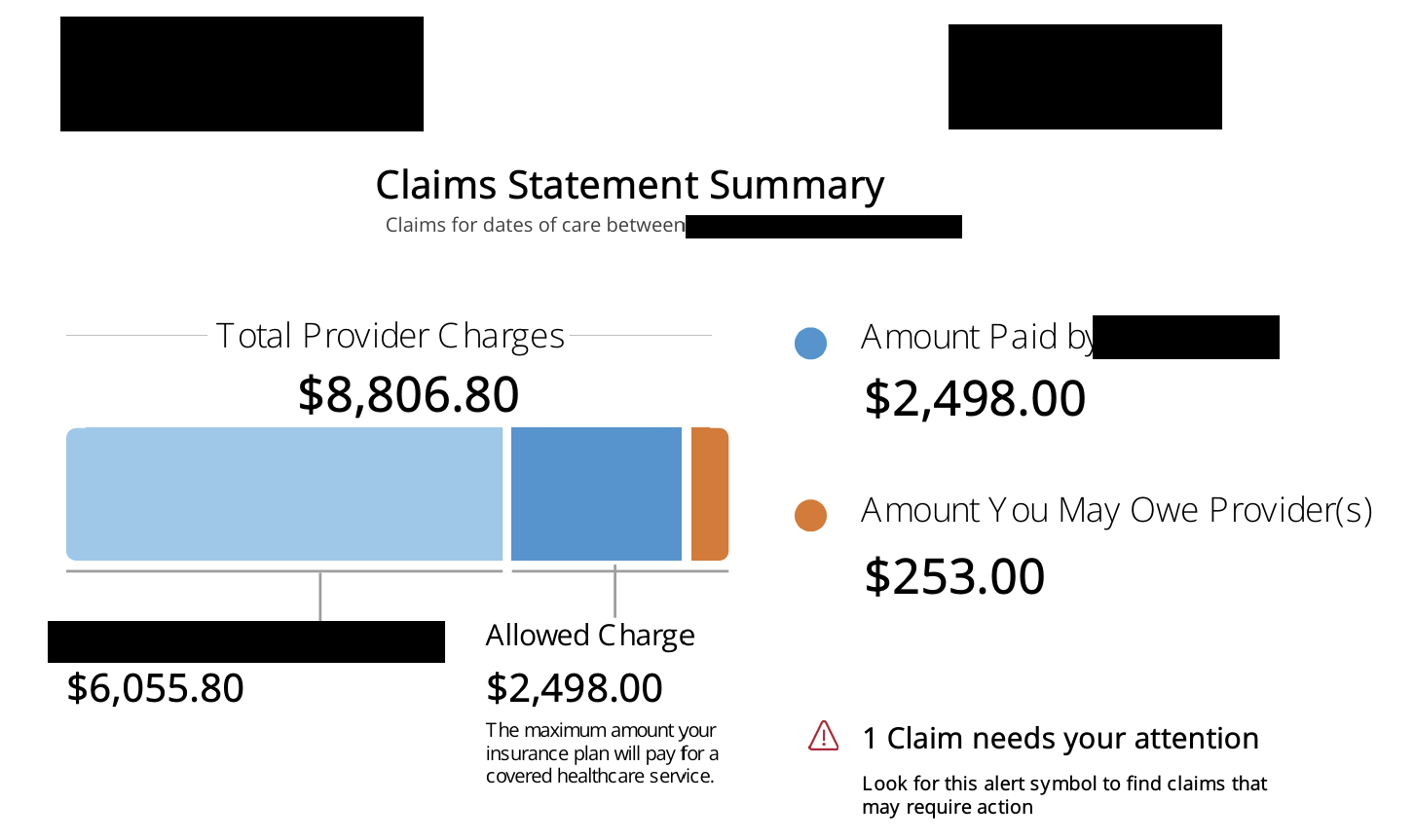
And you get the quote.
$1,500 a month. Per person.
That number hits like a lead balloon. Because nobody — not the business coach, no…
